03 Brachial
typora-copy-images-to: ./images
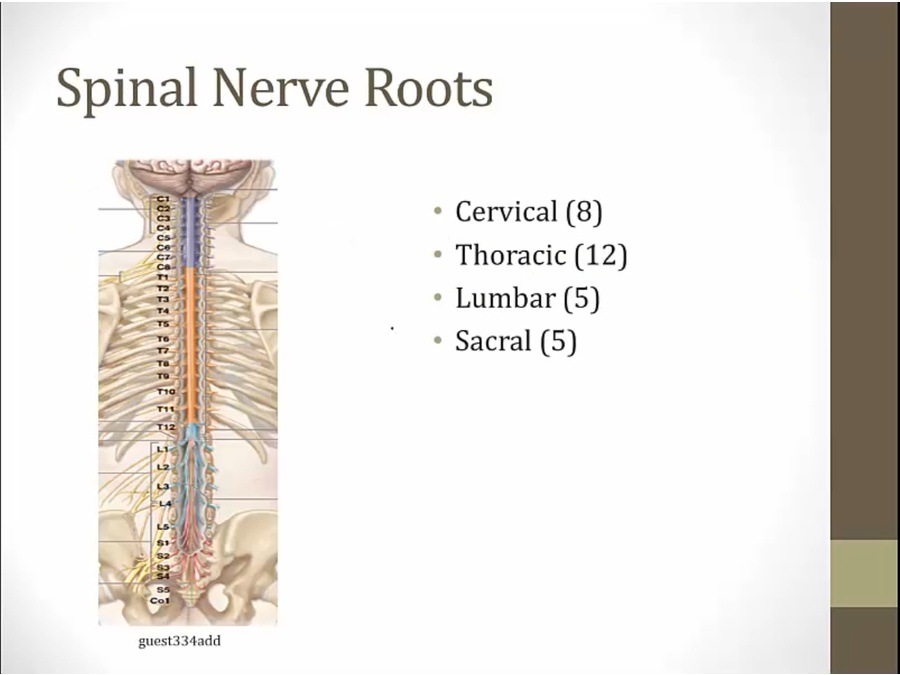
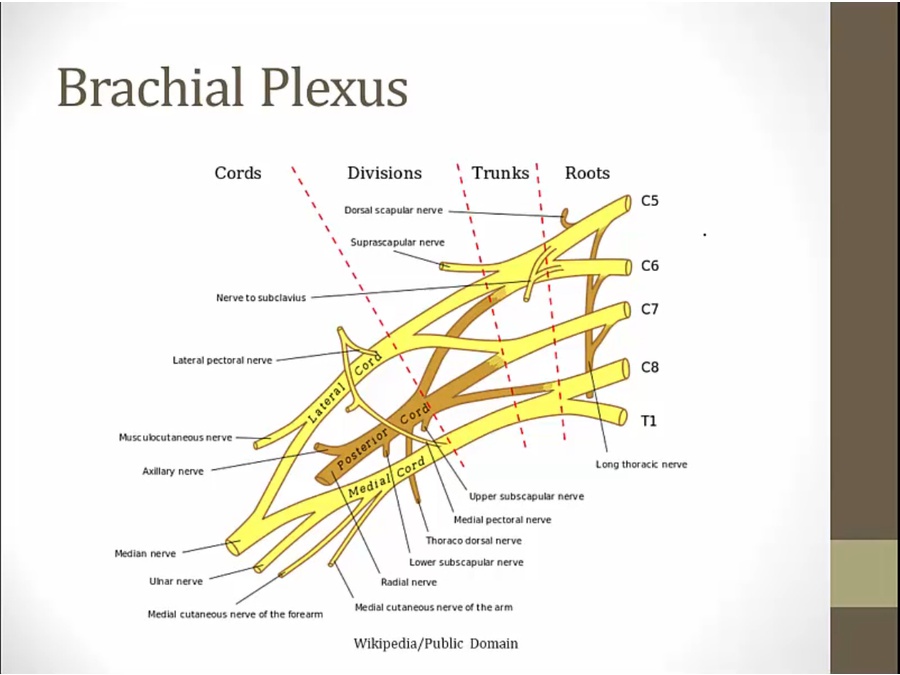
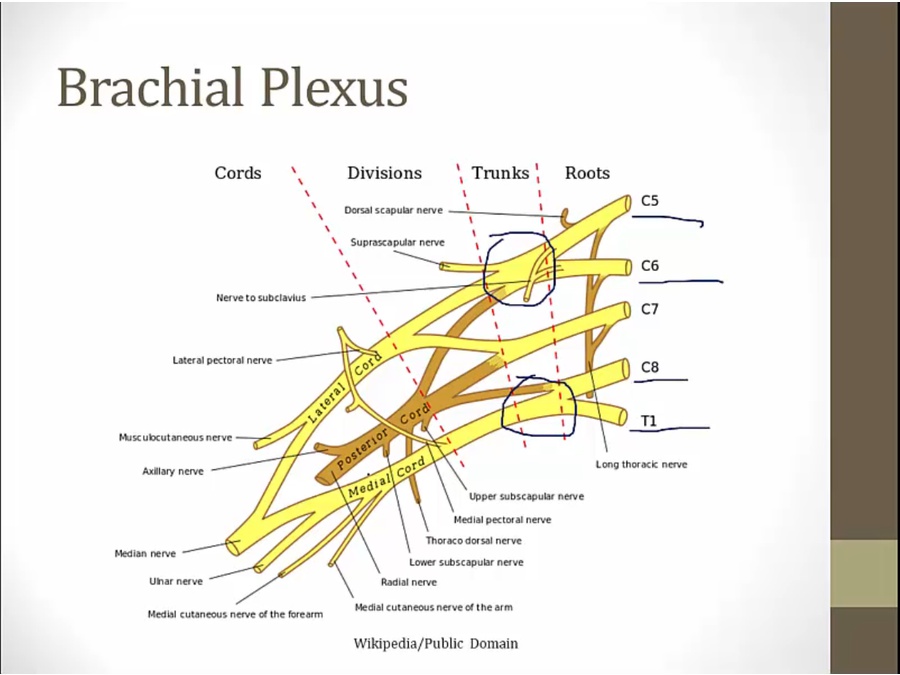
- from spinal cord
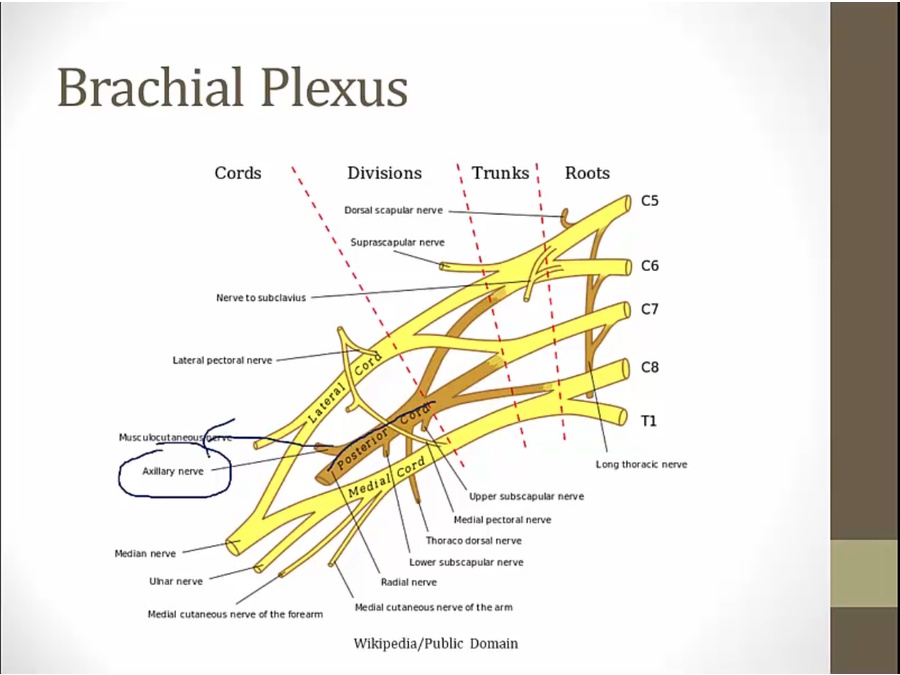
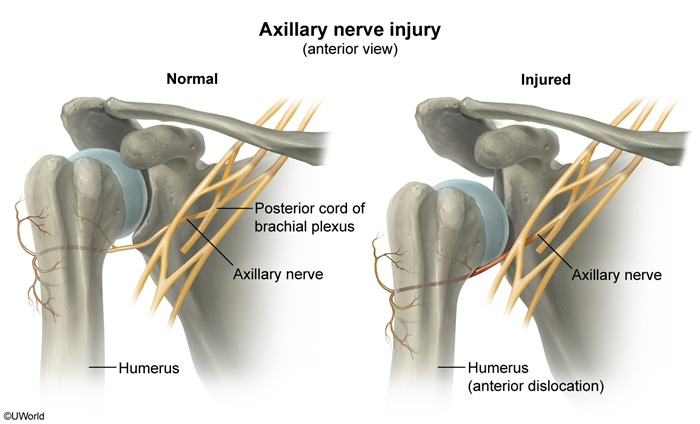
Axillary
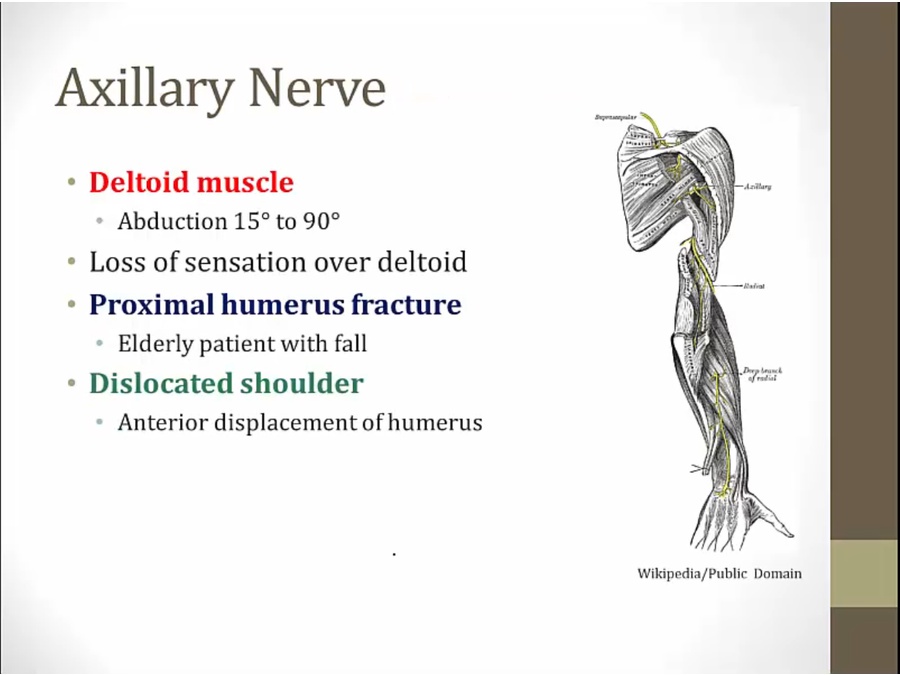
The shoulder may dislocate anteriorly, inferiorly, or posteriorly, but anterior dislocations are by far the most common. Anterior dislocations are typically caused by a blow to an externally rotated and abducted arm.
- from posterior cord, top
- thus mostly C5, C6
Radial
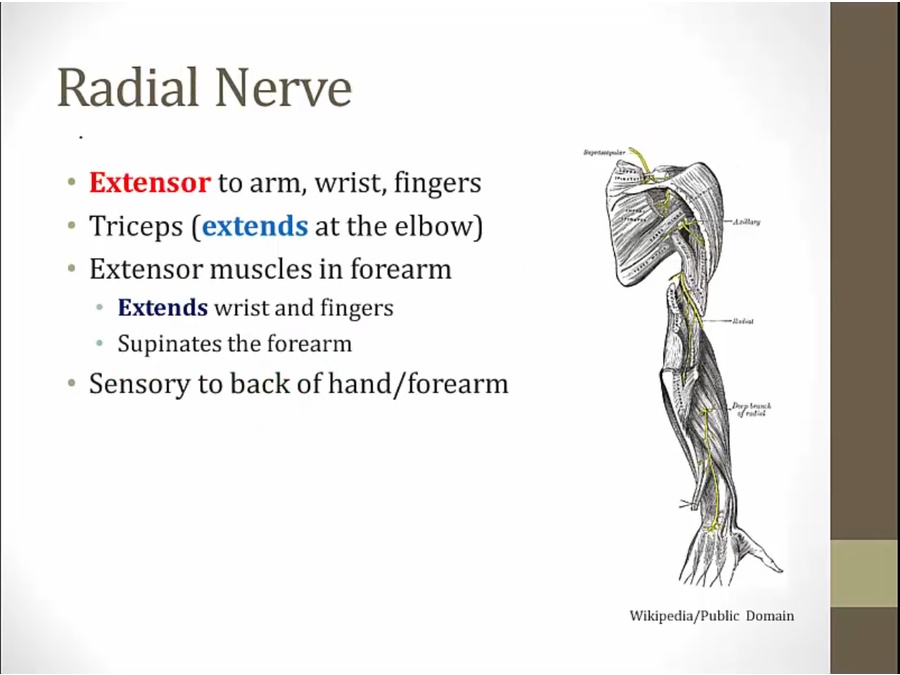
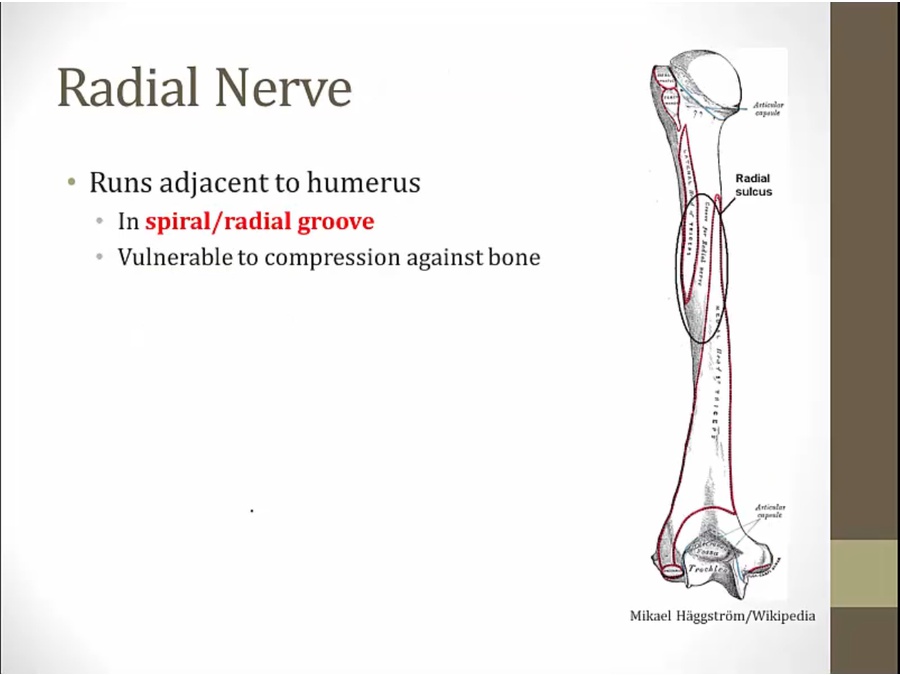
- wraps around humerus, innervates muscles in back of forearm
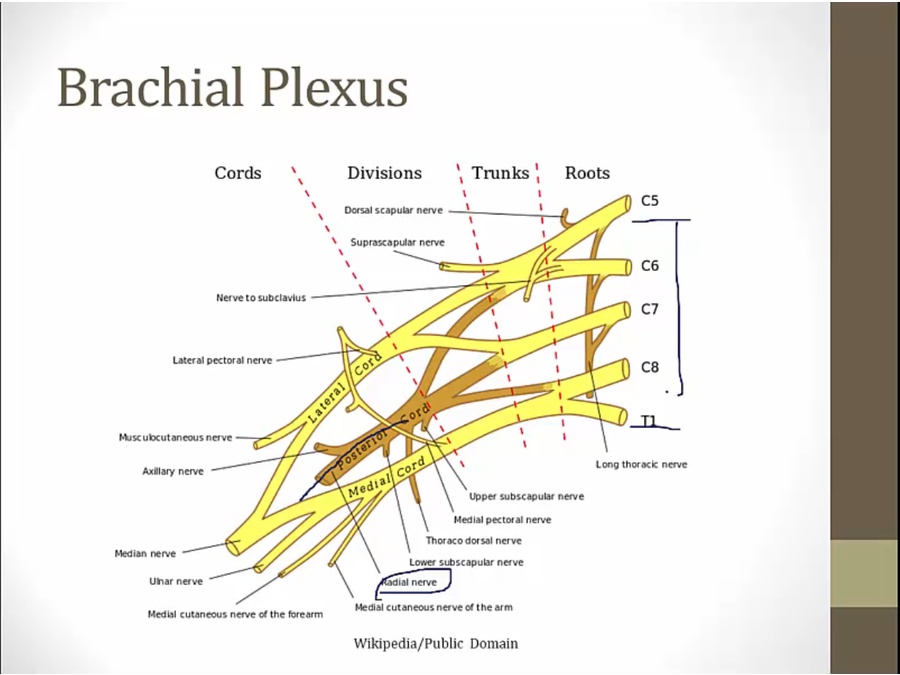
- C5 to T1
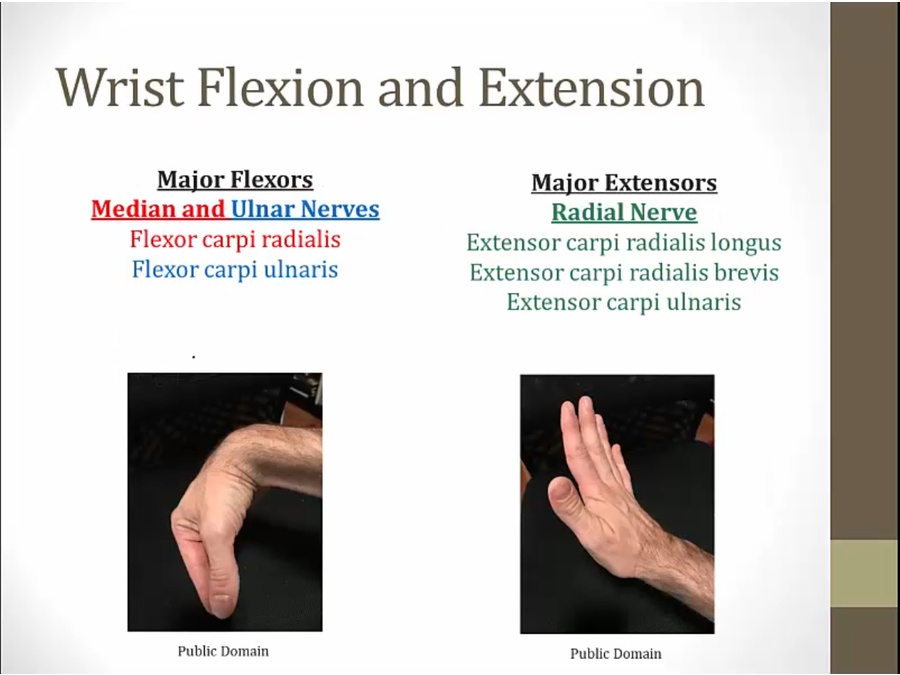
- lose radial nerve, flexors dominate
- wrist drop
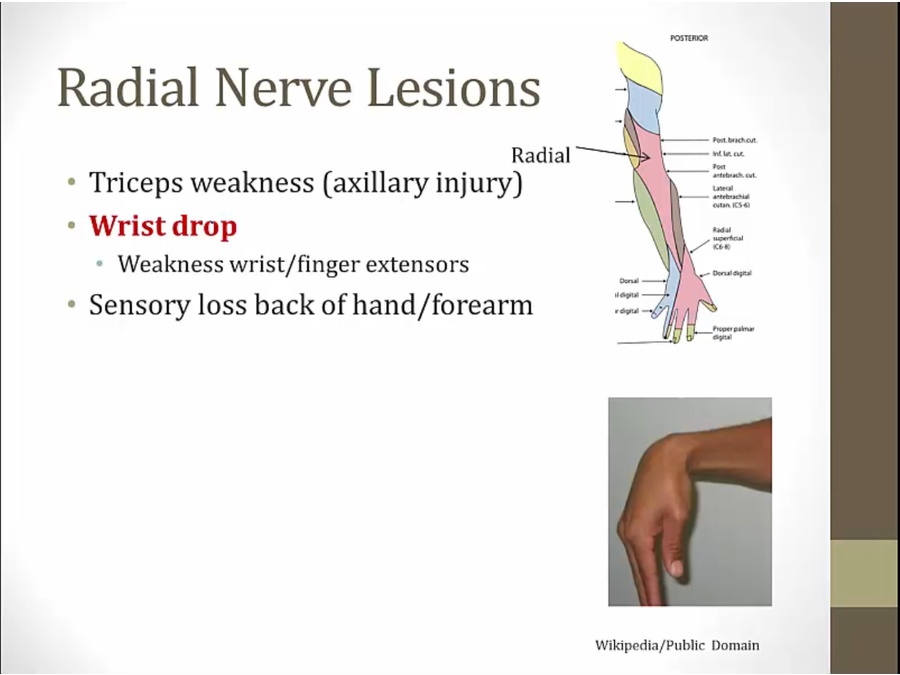
- triceps injury: difficulty extending at elbow
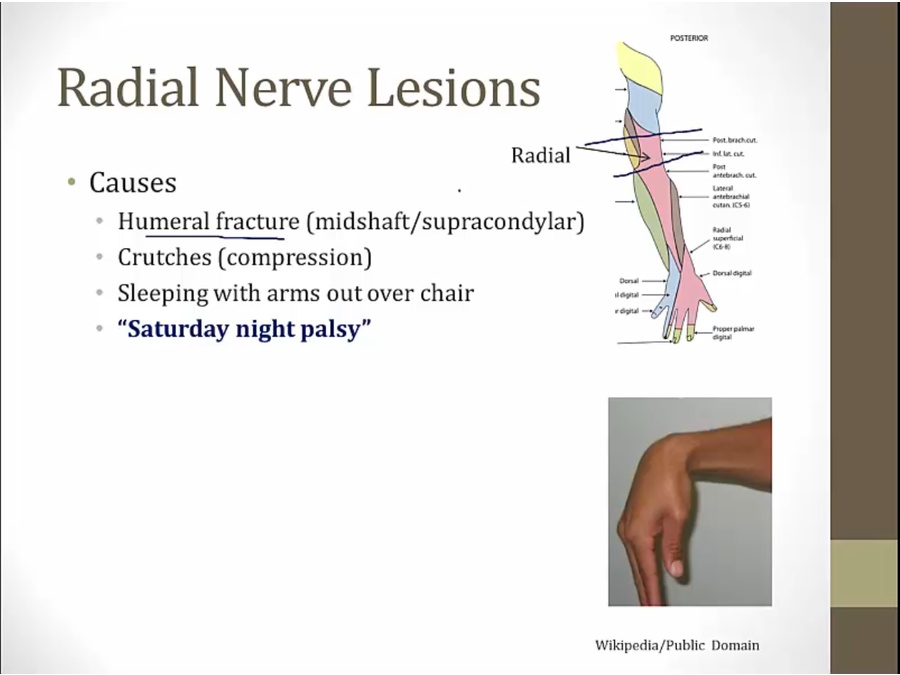
- alcoholics sleep
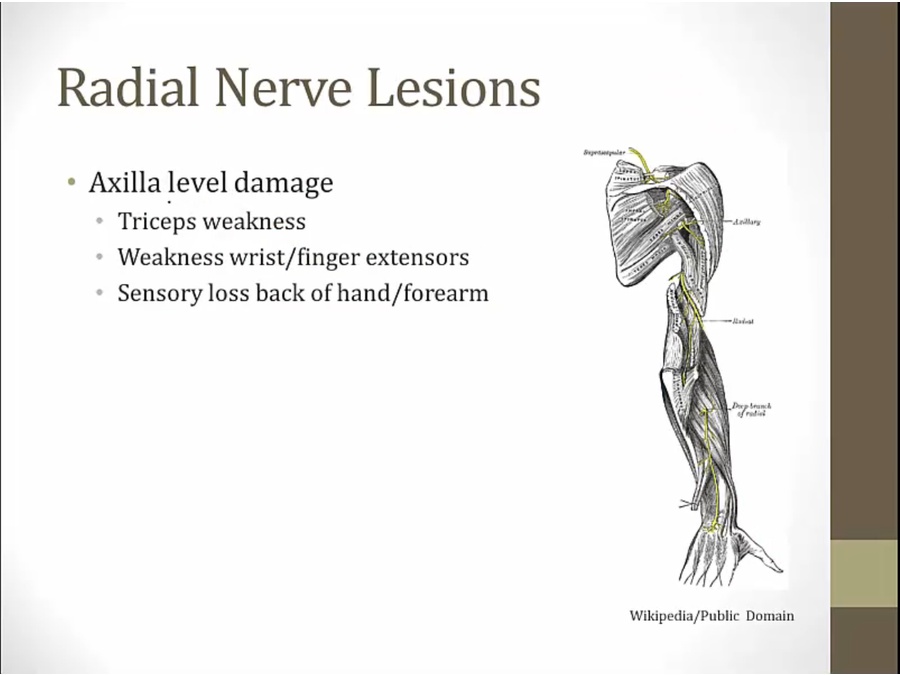
- high up in arm
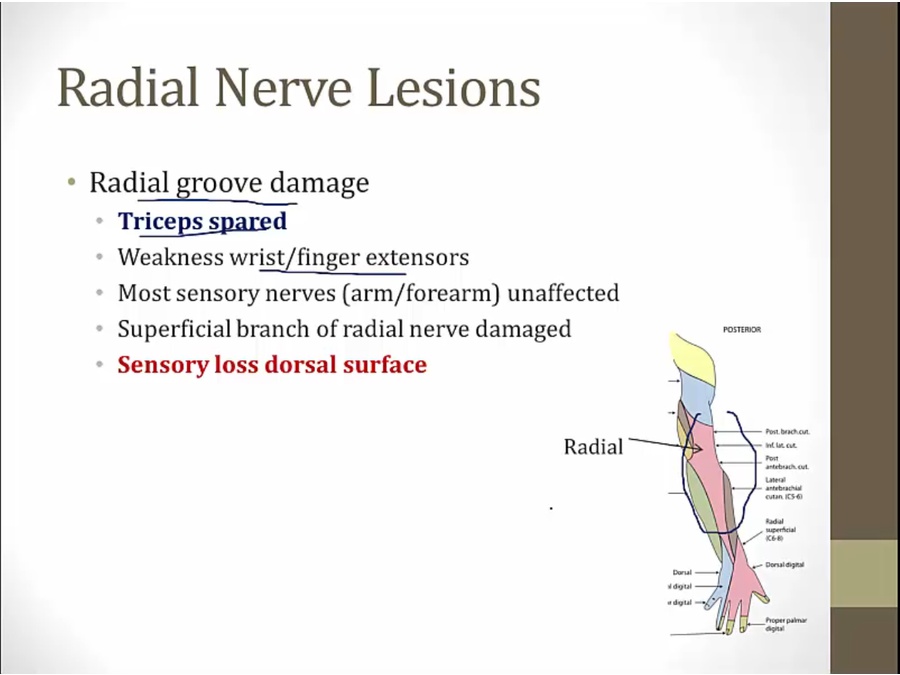
- pink area: sensory by branches given off superficially before
- radial groove damage: normally extension of elbow, loss of extension of wrist/finger, normal sensation of back arm
Ulnar
- most common compression site at medial epicondyle at elbow
Brachial Artery
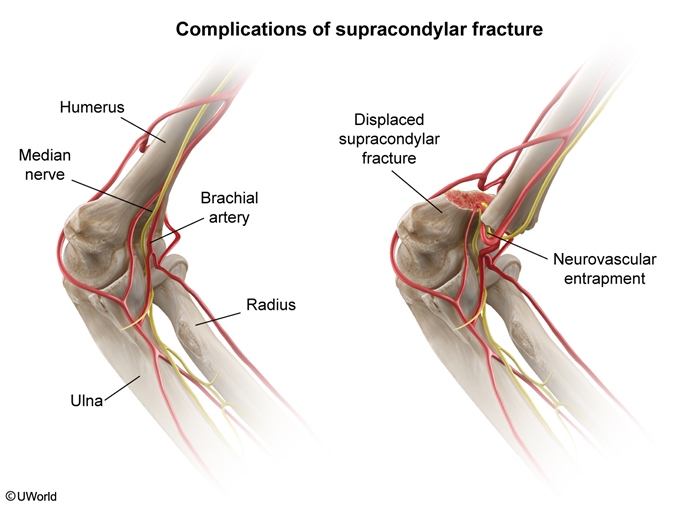
Impingement of the brachial artery results in loss of the brachial and radial artery pulses. Distal perfusion should always be assessed on examination. Motor and sensory function should also be assessed due to the risk of median nerve injury.
Treatment consists of analgesia and immobilization. Displaced fractures require orthopedic consultation. Neurovascular injury often resolves after orthopedic alignment and immobilization; patients who are treated promptly usually have a good prognosis.
Musculocutaneous
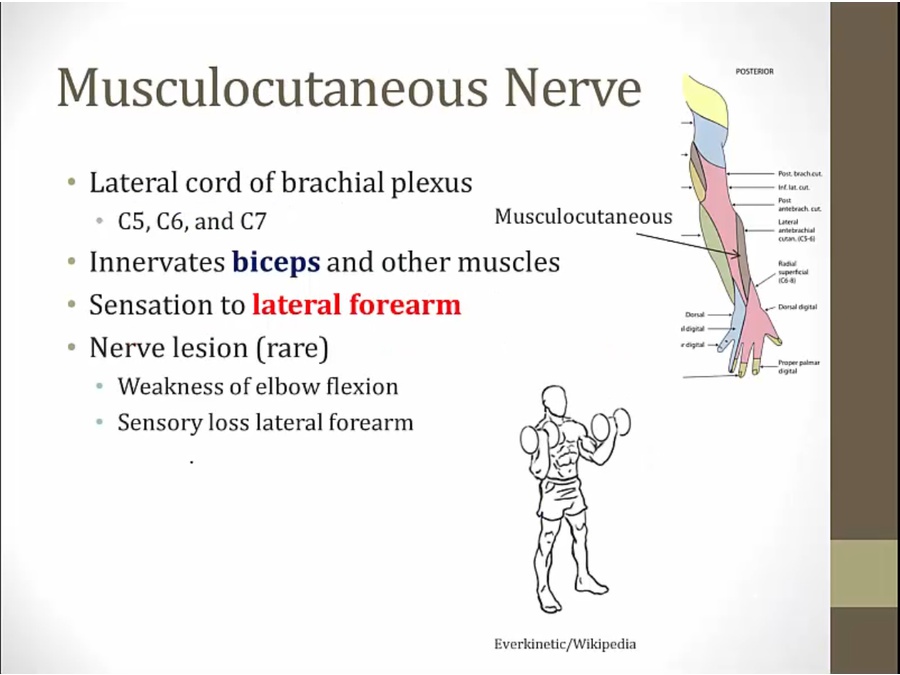
- lateral forearm: thumb side
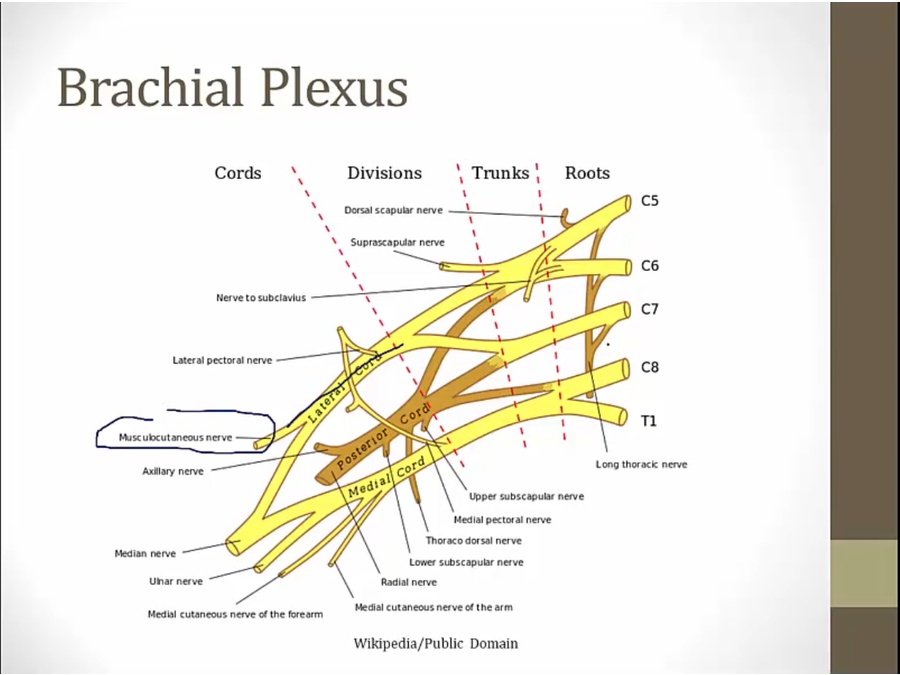
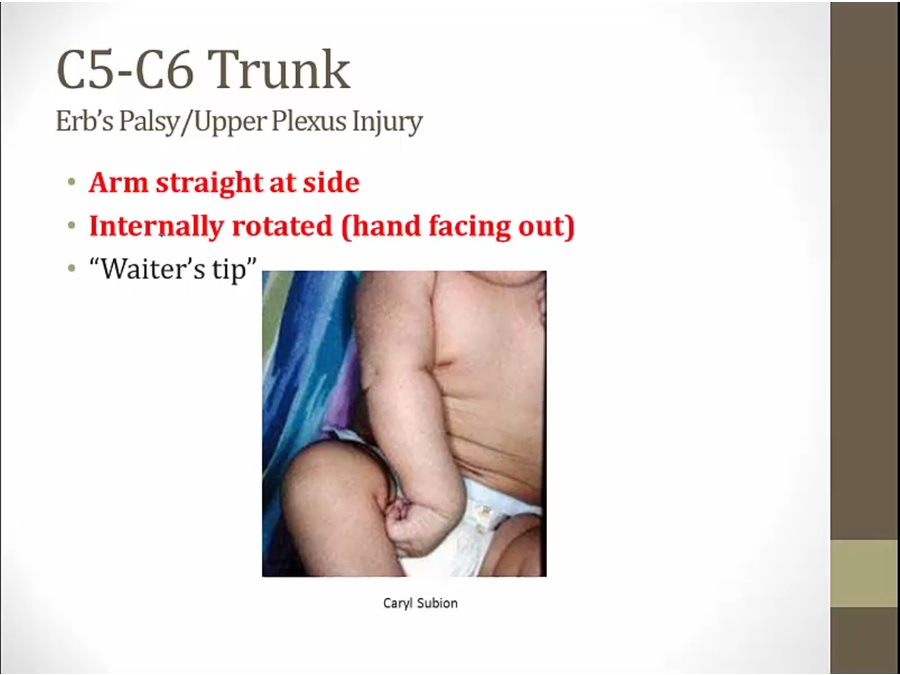
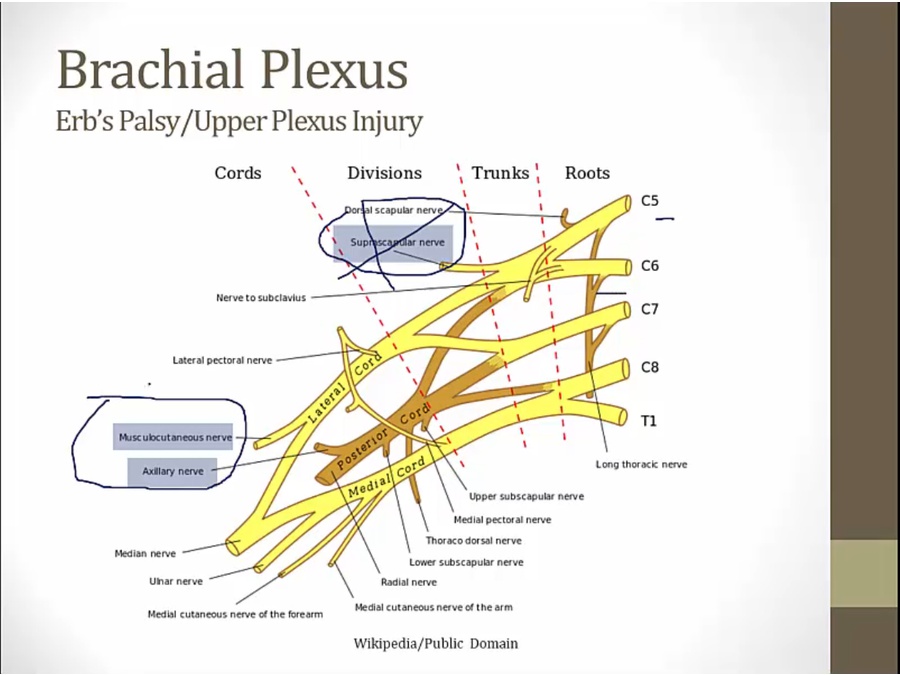
Upper Trunk
- affects nerves derived from upper trunk
Lower Trunk
- arm yanked outwards and upwards
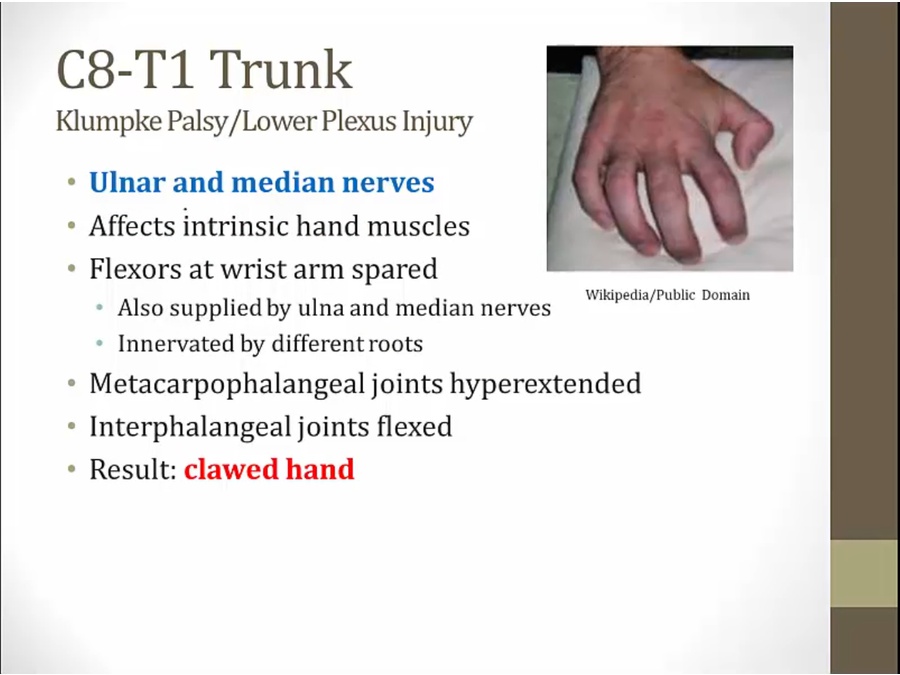
- complete clawed hand
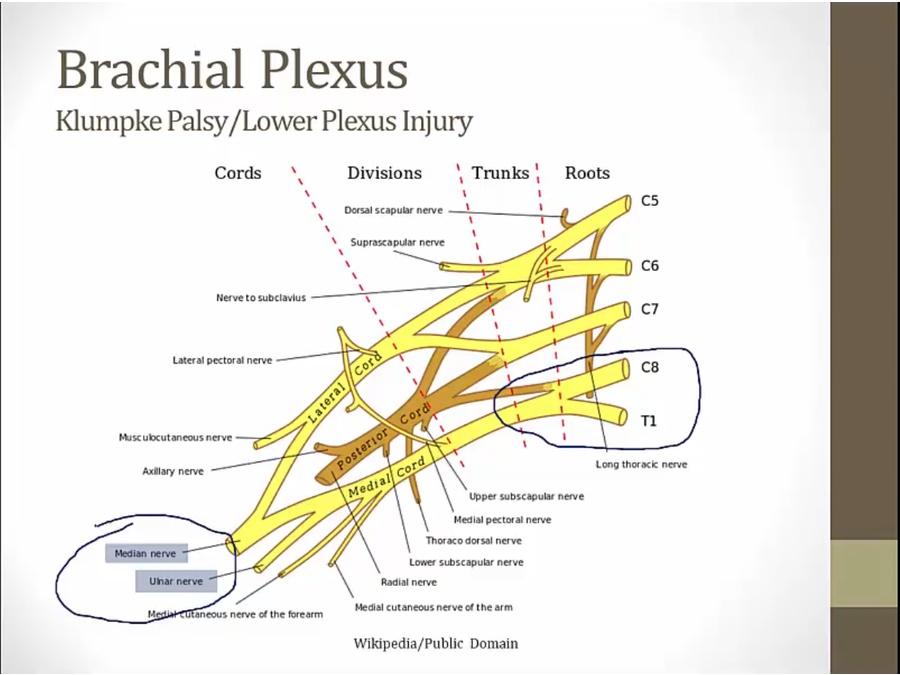
- also some innervation through lateral cord
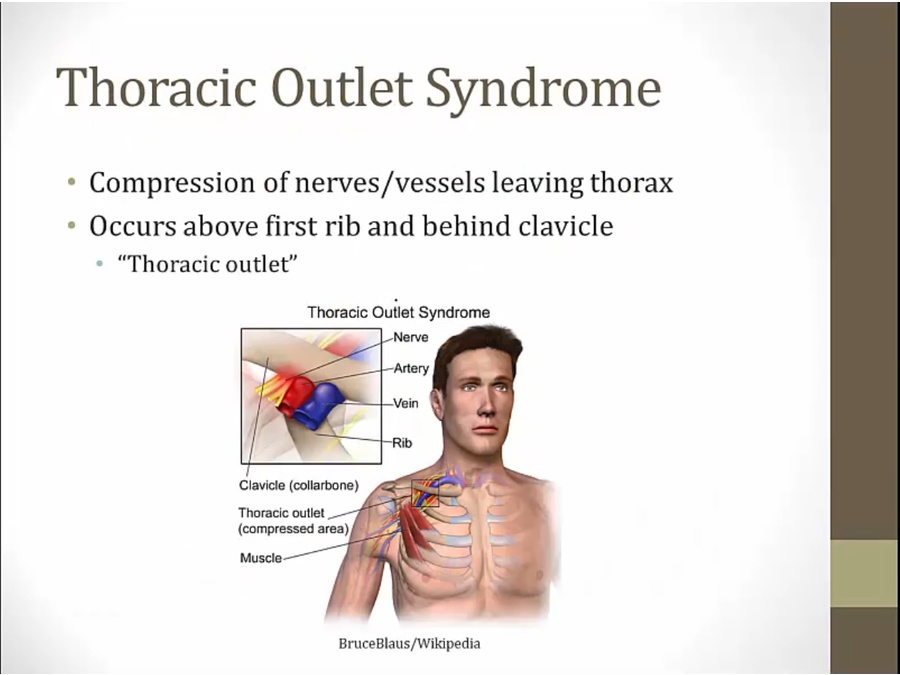
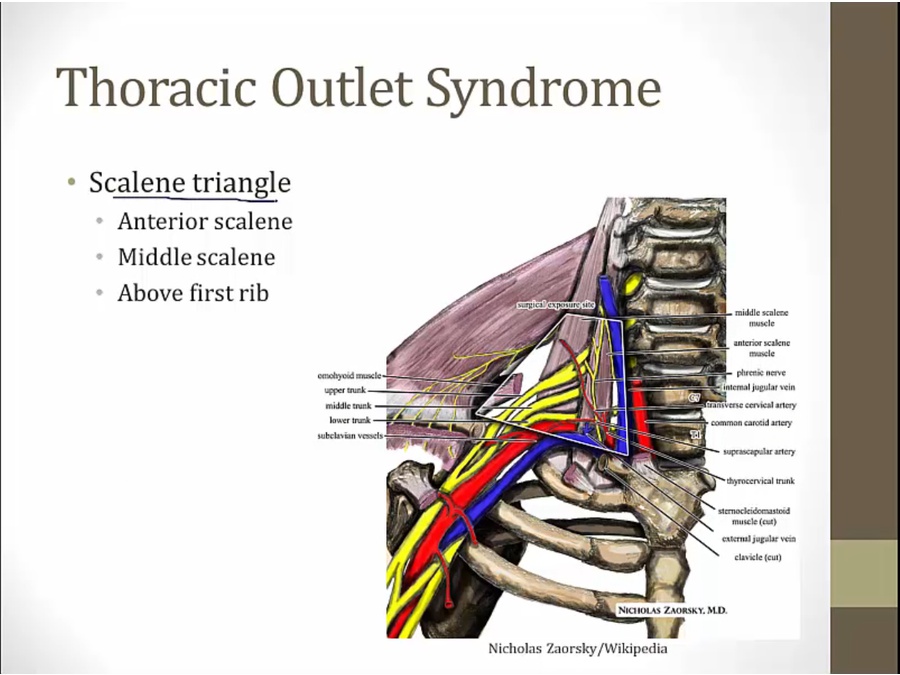
Thoracic Outlet
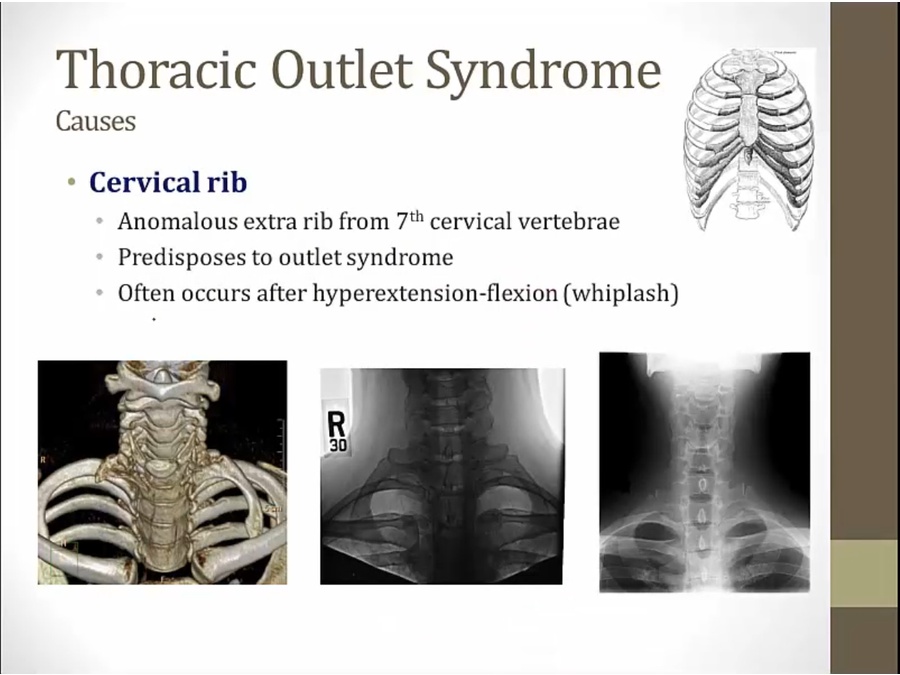
- someone with cervical rib after whiplash
- claw hand
- elevation of arm/hand: compresses nerves more
- elevation of arm: weak pulse
- brachial plexus symptoms plus vasculature symptoms
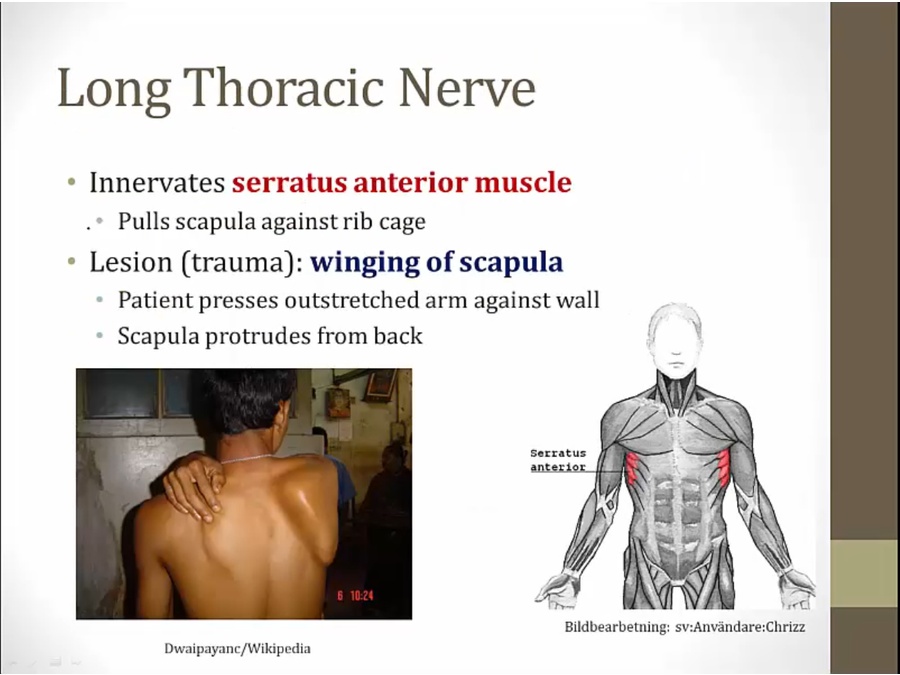
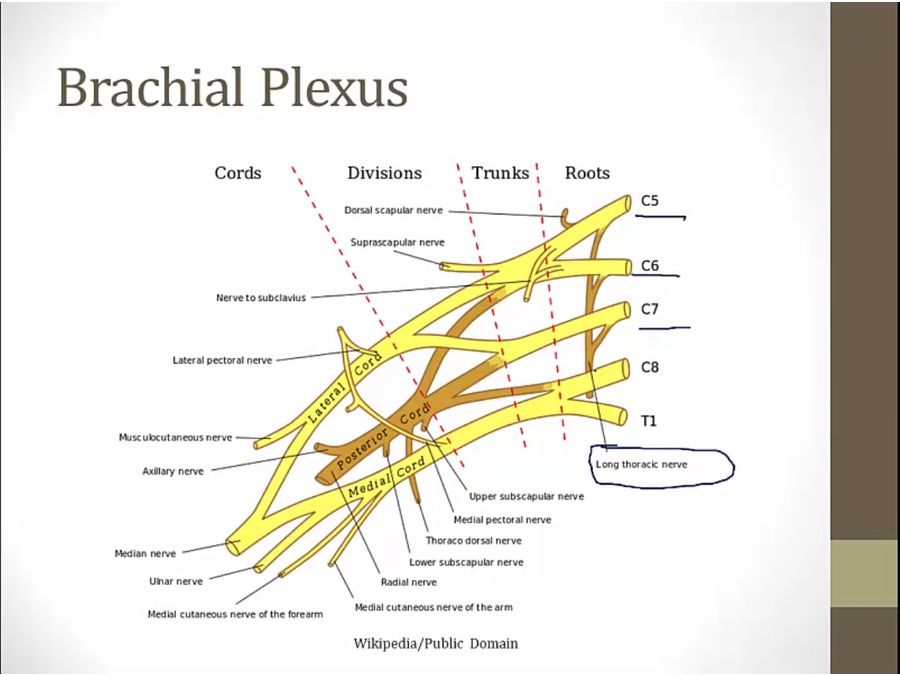
Long Thoracic